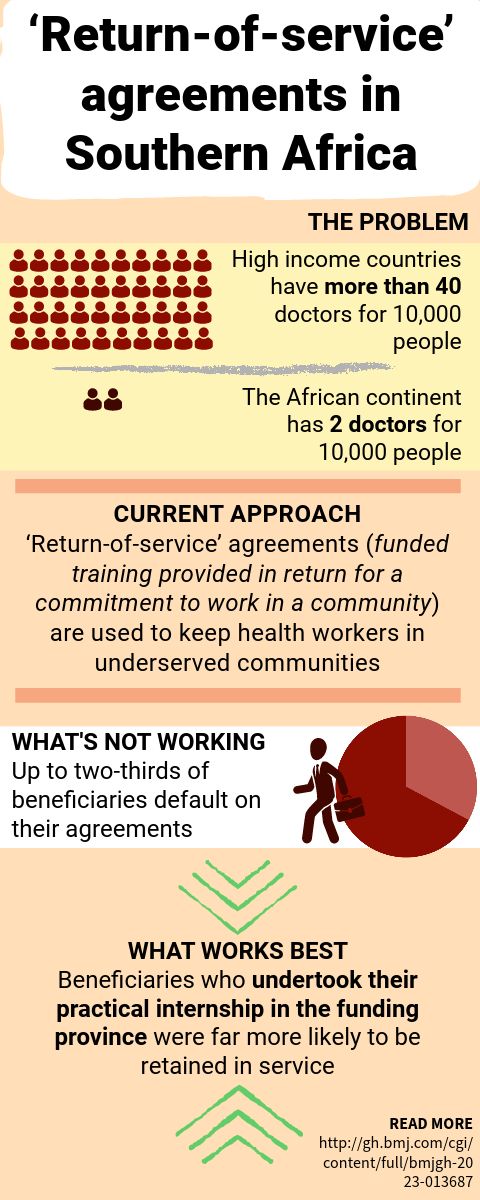
Brain drain in Southern Africa: funded healthcare training programs aren’t keeping workers where they are needed
Researchers find ‘return-of-service’ agreements are not effective in retaining skilled healthcare workers in four Southern African countries, but identify factors for better outcome
Published on the 01 November 2023 by Emily Hogden